
Research Article | DOI: https://doi.org/10.31579/jcitr.2018/004
*Corresponding Author: Matvei Ilya, Department of Radiology, Russia
Citation: Matvei Ilya, Electrophysiological procedures for the use of the RPC: without hindrance and negligible radiation, J. Stem cell Research and Therapeutics International. Doi: 10.31579/jcitr.2018/004
Copyright: © 2018 Matvei Ilya. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 05 September 2018 | Accepted: 17 September 2018 | Published: 24 September 2018
Keywords: radiation exposure; electrophysiological study; dose reduction; fluoroscopy
Background: Fluoroscopy is the main visualization technique for EP procedures. A radiation protection cabin (RPC) shielded with 2 mm lead-equivalent walls was tested as an alternative protection tool (Cathpax®, Lemer Pax).
Methods: To assess the scattered radiation to the operator inside the RPC an electronic personal dosimeter (EPD; Mk2, Thermo Electron) was placed at the neck level of the operator. A second EPD was located outside the RPC at 150 cm height from the floor, to record the presumable head radiation dose.
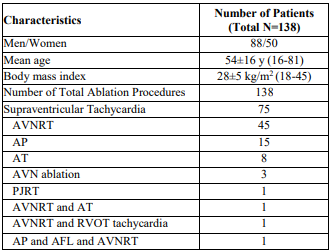
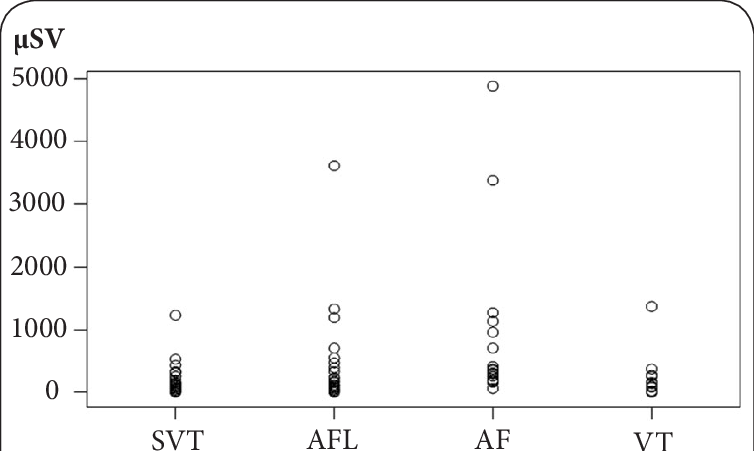
Results: Radiation doses were measured in a total of 138 consecutive patients (age 54±16 yrs, BMI 28±5 kg/m2 (18-45), 64% male) undergoing a variety of ablation procedures (SVT=75, AFL=32, AF=17, VT=14). Median fluoroscopy time was 39 min (7-140), the cumulative dose-area product (DAP) 4702 cGy.cm2 (493-65620). Doses outside the RPC showed a median of 135 µSv (1-4881). Doses inside the RPC were detected only at sensitivity threshold or background levels (mean 0.2SD0.7 µSv, median 0.0, range 0-4). The dose reduction to the operator was highest for AF ablations (354 vs 0.5 µSv, respectively; p<0.001). The total accumulated dose outside the RPC was 37883 µSv for all 138 procedures, whereas for the protected operator inside only 30 µSv.
Conclusions: There were highly concordant low dose values measured for the operator inside the RPC in comparison to high doses outside the RPC. The use of a RPC represents a major benefit over a lead apron and contributes to a significant dose reduction as low as reasonably achievable (ALARA principle).
Despite introduction of three-dimensional mapping and improved ablation technology, fluoroscopy will remain the main visualization technique for electrophysiological (EP) procedures. Furthermore, the complexity and the volume of invasive EP studies have substantially increased over the last decades. Especially ablation of atrial fibrillation (AF) is a complex and prolonged procedure and associated with high radiation doses due to prolonged fluoroscopy times of more than 120 minutes depending on anatomic variations and operator experience [1,2]. High cumulative radiation exposure of the operator may result in potential stochastic and deterministic sequels [3-5]. Traditional radiation protection with lead aprons, goggles, and a thyroid shield leaves unprotected body parts such as arms, hands and head. Moreover, lead aprons are heavy and uncomfortable for the operator during prolonged procedures. In this study a radiation protection cabin (RPC) (Cathpax®, Lamer Pax, Carquefou, France) shielded with 2 mm lead-equivalent walls was tested as an alternative protection tool (Figure 1). The RPC is mobile, adjustable in height, and is prepared with specifically designed drapes to provide sterile patient access. The main objective was the comparison of radiation doses inside the RPC versus outside the RPC for different ablation procedures.

Methods
The X-ray system used for EP procedures was a biplane (83% of cases) or monoplane Philips Allura Xper FD10 system (Philips Healthcare; DA Best, The Netherlands). Pulsed low frame fluoroscopy (7.5 frames per second) and entrance dose limitation were used for air kerma reduction. The tubes of both systems have integrated dose-area product (DAP) meters indicating the cumulative DAP in cGy.cm2 of each interventional procedure. DAP is a surrogate marker for the total amount of radiation energy delivered to the patient, hence serving as a relative indication of the scatter-dose to the operator.
To assess the scattered radiation to the operator inside the RPC an electronic personal dosimeter (EPD Mk2, Thermo Fisher Scientific, Waltham, MA) was placed at the back of the neck of the operator (Figure 1). A second EPD was located outside the RPC on the left-sided lateral wall of the cabin, at 150 cm height from the floor (Figure 2), to record the presumable head radiation dose. Dose display and storage of the EPD Mk2 ranges from 0 µSv to >16 Sv (auto ranging) at a resolution of 1 µSv up to 10 mSv.

All ablation procedures were performed with the RPC in use without compromising catheter manipulations of the operator. To gain access to both femoral veins and the right jugular vein all vessel punctures and the introduction of sheaths were performed before placement of the cabin.
The study compromised a total of 138 consecutive ablation procedures (supraventricular tachycardia (SVT) = 75, atrial flutter (AFL) = 32, atrial fibrillation (AF) = 17, ventricular tachycardia (VT) = 14. Mean age of the patients was 54±16 years, body mass index 28±5 kg/m2 (range 18-45), 64% men (Table 1). Median fluoroscopy time was 39 min (range 7-140). The externally applied radiation energy per minute fluoroscopy, as measured by the cumulative DAP was 4702 cGy.cm2 (range 493-65620). Doses outside the RPC showed a median of 135 µSv (range 1-4881). In 9/138 ablations (6.5%) doses were >1000 µSv/procedure, indicating a high exposure to the head (Figure 3). Doses inside the RPC were detected only at sensitivity threshold or background levels (mean 0.2SD0.7 µSv, median 0.0, range 0-4) (Figure 4). The dose reduction to the operator was highest for AF ablations when comparing values outside versus inside the cabin (354 versus0.5 µSv, respectively; p<0.001). The total accumulated dose outside the RPC was 37883 µSv for all 138 procedures, whereas for the protected operator inside only 30 µSv.

The present study demonstrates that the use of the RPC significantly reduces the radiation dose to the invasive electro physiologist as low as reasonably achievable (ALARA principle). The dose values measured for the operator inside the cabin were concordant low among all procedures. Our data are in line with the findings by Dragusin et al., [6] who demonstrated the usefulness of the RPC cabin compared to traditional radiation protection. In contrast to the cited study, we used a biplane X-ray system for the majority of ablation cases (>80%), whereas Dragusin et al., reported the use of a monoplane system in 70% of the procedures. As a major difference the French and Belgian investigators compared electrophysiological procedures with protection provided by classical means (lead apron) versus the RPC. Doses were measured with either thermoluminiscent or electronic dosimeters at multiple sites in protected and unprotected areas, whereas in our study all procedures were performed with the operator behind the RPC using only two EPDs, one inside the other outside the RPC. This setting was chosen in light of the results of the previously published study that found significant differences between conventional protection and the RPC particularly for radiation exposure to the head and neck of the operator. However, the different fluoroscopic systems, types of ablation and measurement techniques in both studies preclude a direct comparison of doses. Nevertheless, our findings confirm the significant reduction of radiation dose particularly to unprotected areas of the body that can be achieved using the RPC in a variety of more or less complex electrophysiological procedures.
Renaud [7] reported an annual dose exposure to the head of invasive cardiologist in the range of 20-30 mSv per year. Furthermore there are data indicating an increased risk of brain tumors in medical radiation workers because of absence of head protection [4]. In the present study the electronic dosimeter outside the cabin was placed in a way to record the presumable head radiation dose. The doses measured outside the cabin indicate that EP operators are exposed to relatively high radiation levels without shielding, particularly to the regions of the head and neck. Dose values inside the cabin were negligible low. Therefore, the dose reduction with the RPC, covering head and arms, certainly represents a benefit over the use of conventional radioprotection, such as lead aprons, a lead glass screen or lead eye glasses [8].
Over the last decade the number of AF ablations has dramatically increased and the trend is likely to continue in the future. AF ablation procedures are complex, prolonged and associated with larger radiation doses [1,2]. Lickfett and coworkers reported a fourfold increase in fluoroscopic screening time for AF ablations compared to AFL ablations and an eightfold increase compared to AVNRT ablation procedures [2]. The present study confirmed this finding and documented high radiation doses, particularly for complex AF ablations. Consequently, the dose reduction to the operator was highest for left atrial ablation procedures.
The work behind the RPC is much more comfortable compared to wearing a heavy lead apron, especially during prolonged procedures. Long-term orthopaedic problems are increasing in interventional cardiologists due to heavy lead aprons [9-11]. The use of the RPC on a routine basis might prevent such orthopaedic problems. However, the RPC has been designed mainly for electrophysiological procedures and until now there are no comparable protection systems available for coronary interventions or device implantations. In our experience, the RPC did not pose any hindrances to the operator with respect to catheter manipulation or even transseptal puncture for left atrial ablations. However, repositioning of the coronary sinus catheter from above was possible only form outside the RPC. Over the last years the regular use of the RPC has become routine in our EP laboratory independent of the type of the procedure. The consistent use of the RPC will ensure that individual dosimetry of high-volume operators will remain far below the upper recommended annual effective dose limit of 20mSv per year in our country.
The use of the RPC allowed the operators to perform a variety of catheter ablations without hindrance and negligible radiation. There were highly concordant low dose values measured inside the RPC over a clinically relevant wide spectrum of procedures. The doses measured outside the RPC confirm that electrophysiologists are exposed to relatively high dose levels, particularly during AF ablations. Use of a RPC represents a major benefit over a lead apron and contributes to a significant dose reduction as low as reasonably achievable (ALARA principle).
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
